A 60-year-old female presents to the emergency department complaining of intense left sided-flank pain radiating to the groin. Urinalysis is positive for gross hematuria, while a non-contrast CT of the abdomen and pelvis is negative for stones.
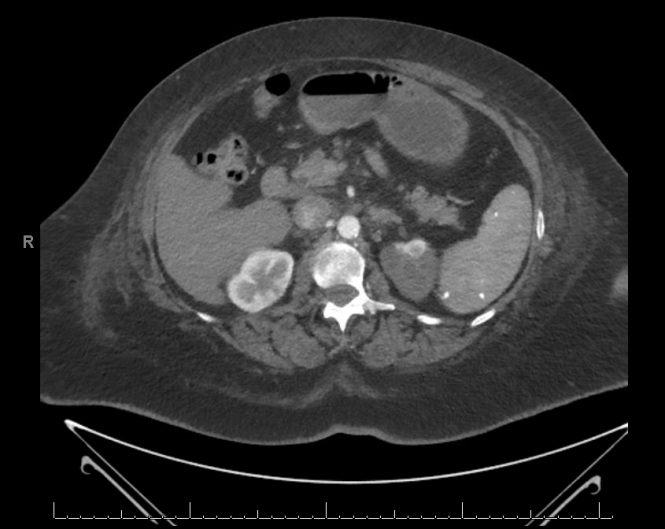
The patient is sent for a contrast CT of the abdomen and pelvic, from which the following image is taken:

The patient was then re-examined at the bedside and her pulse was noted to be abnormal.
Question 1: What pulse abnormality would most likely account for the finding in the above image and why?
Question 2: What serum laboratory abnormality, if strongly positive, would best support this patient’s CT-evidenced diagnosis?
(Question 1 already answered and awarded per below. The Medical Media Review will give a $100 Amazon.com gift card to whoever posts the correct answer to Question 2 first. Offer expires August 31, 2015. See Contest Rules for additional details.)

Leave a Reply